Specialized Staff for the Care of People with Parkinson’s Disease in Germany: An Overview

 ,
,  , , , ,
, , , ,
Abstract
:1. Background
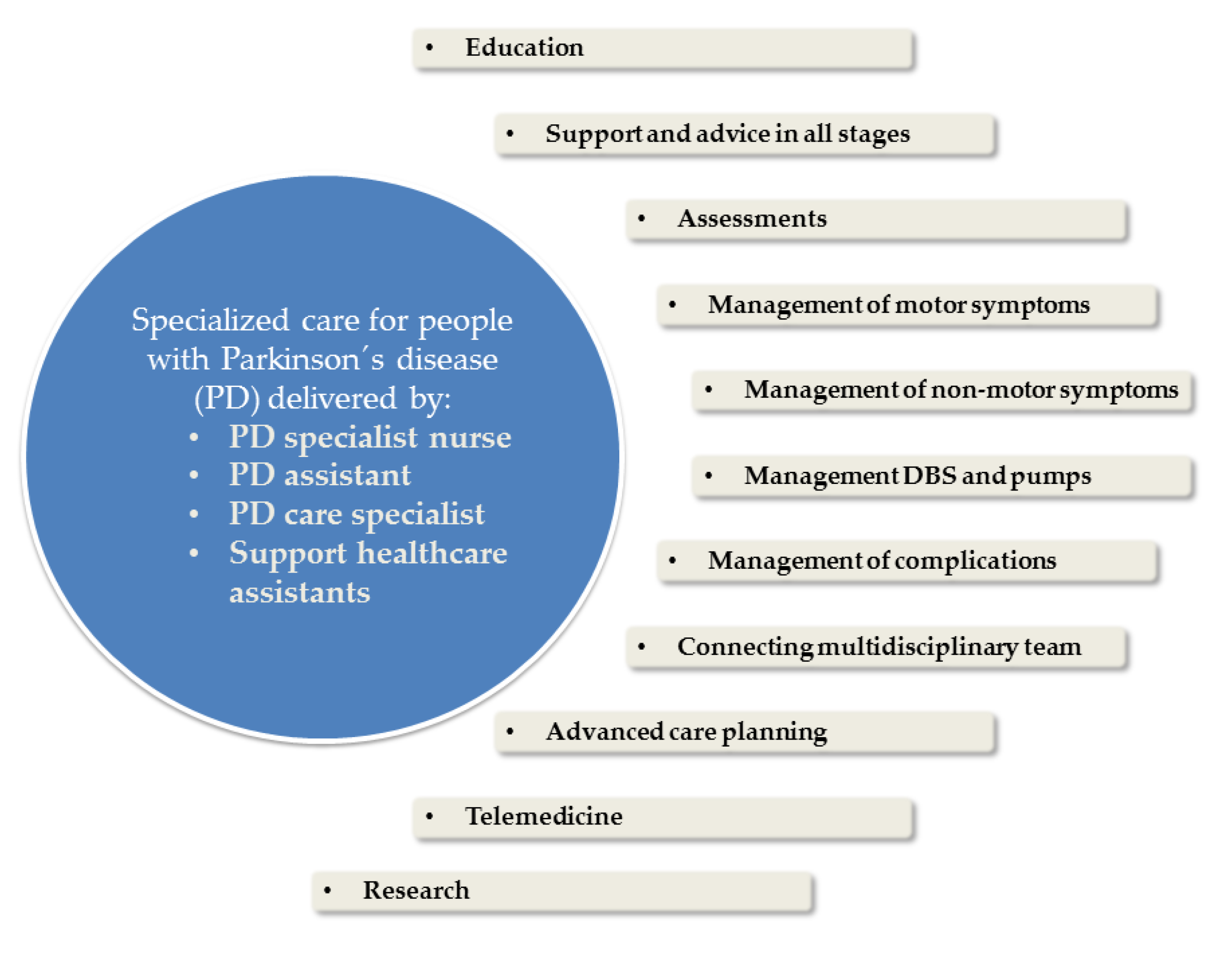
2. Field of Activities and Responsibilities
- Help to cope with PD, answer frequent and everyday questions and give advice where doctors lack the necessary time: Typical questions are for example “What do I have to pay attention to with the medication?”, “Can I go on holiday?”, or “Can I do sports?”
- Use assessments to identify and monitor symptoms, side effects, and family problems
- Advise on the motor and NMS and complications.
- Counsel relatives and monitor their burden
- Teach other health and social care professionals (e.g., for handling pumps or deep brain stimulation (DBS))
- Inform comprehensively about therapy options, self-help groups or socio-medical aspects, such as applying for care levels or certificates for severely disabled persons
- Help to improve adherence to medication
- Assist in the initiation and adjustment of continuous therapies or take over most of them independently
- Support in making the PD diagnosis (e.g., performing an L-dopa or apomorphine challenge test)
- Make referrals to other professionals such as speech and language therapists, occupational therapists, physiotherapists or social workers and support networking between different therapeutic players
- Assist in advanced care planning (ACP)
3. Parkinson’s Disease Nurse Specialist (PD Nurse)
4. Parkinson Assistant (PASS Concept)
5. Parkinson Care Specialist (Parkinson Pflegespezialist/In)
6. Support of Health Care Assistants in General Practice and Outpatient Clinics
7. Community Matrons
8. Proposal of Core Elements for Future PDS Education in Germany
9. Concluding Remarks
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22, S119–S122. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Feldmann, F.; Zipprich, H.M.; Witte, O.W.; Prell, T. Self-Reported Nonadherence Predicts Changes of Medication after Discharge from Hospital in People with Parkinson’s Disease. Parkinsons Dis. 2020, 2020, 4315489. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Bartig, D.; Muhlack, S.; Hartelt, E.; Scherbaum, R.; Katsanos, A.H.; Muller, T.; Jost, W.; Ebersbach, G.; Gold, R.; et al. Dynamics of Parkinson’s Disease Multimodal Complex Treatment in Germany from 2010–2016, Patient Characteristics, Access to Treatment, and Formation of Regional Centers. Cells 2019, 8, 151. [Google Scholar] [CrossRef] [Green Version]
- Müller, T.; Öhm, G.; Eilert, K.; Möhr, K.; Rotter, S.; Haas, T.; Küchler, M.; Lütge, S.; Marg, M.; Rothe, H. Benefit on motor and non-motor behavior in a specialized unit for Parkinson’s disease. J. Neural Transm. 2017, 124, 715–720. [Google Scholar] [CrossRef]
- Scherbaum, R.; Hartelt, E.; Kinkel, M.; Gold, R.; Muhlack, S.; Tonges, L. Parkinson’s Disease Multimodal Complex Treatment improves motor symptoms, depression and quality of life. J. Neurol. 2019, 267. [Google Scholar] [CrossRef]
- Gerlach, O.H.; Winogrodzka, A.; Weber, W.E. Clinical problems in the hospitalized Parkinson’s disease patient: Systematic review. Mov. Disord. 2011, 26, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.; Fry, M. The utilisation of one district hospital emergency department by people with Parkinson’s disease. Australas. Emerg. Nurs. J. 2017, 20, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Okunoye, O.; Kojima, G.; Marston, L.; Walters, K.; Schrag, A. Factors associated with hospitalisation among people with Parkinson’s disease-A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2020, 71, 66–72. [Google Scholar] [CrossRef]
- Vossius, C.; Nilsen, O.B.; Larsen, J.P. Parkinson’s disease and nursing home placement: The economic impact of the need for care. Eur. J. Neurol. 2009, 16, 194–200. [Google Scholar] [CrossRef]
- Binder, S.; Groppa, S.; Woitalla, D.; Müller, T.; Wellach, I.; Klucken, J.; Eggers, C.; Liersch, S.; Amelung, V.E. Patients’ Perspective on Provided Health Services in Parkinsonʼs Disease in Germany—A Cross-Sectional Survey. Akt Neurol. 2018, 45, 703–710. [Google Scholar]
- Hellqvist, C.; Bertero, C. Support supplied by Parkinson’s disease specialist nurses to Parkinson’s disease patients and their spouses. Appl. Nurs. Res. 2015, 28, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Lennaerts, H.; Groot, M.; Rood, B.; Gilissen, K.; Tulp, H.; van Wensen, E.; Munneke, M.; van Laar, T.; Bloem, B.R. A Guideline for Parkinson’s Disease Nurse Specialists, with Recommendations for Clinical Practice. J. Parkinsons Dis. 2017, 7, 749–754. [Google Scholar] [CrossRef] [PubMed]
- MacMahon, D.G. Parkinson’s disease nurse specialists: An important role in disease management. Neurology 1999, 52, S21–S25. [Google Scholar] [PubMed]
- Osborne, L. Marking 20 years of Parkinson’s disease nurse specialists: Looking to the future. Br. J. Neurosci. Nurs. 2013, 5, 450–455. [Google Scholar] [CrossRef]
- Axelrod, L.; Gage, H.; Kaye, J.; Bryan, K.; Trend, P.; Wade, D. Workloads of Parkinson’s specialist nurses: Implications for implementing national service guidelines in England. J. Clin. Nurs. 2010, 19, 3575–3580. [Google Scholar] [CrossRef] [Green Version]
- German Society of Neurology (DGN). S3 Leitlinie Idiopathisches Parkinson Syndrom. Available online: https://www.deutsche-apotheker-zeitung.de/daz-az/2016/daz-17-2016/leitlinien-update-morbus-parkinson (accessed on 29 June 2020).
- Titova, N.; Chaudhuri, K.R. Personalized Medicine and Nonmotor Symptoms in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 134, 1257–1281. [Google Scholar]
- A competency Framework for Nurses Working in Parkinson’s Disease Management. Available online: https://www.parkinsons.org.uk/sites/default/files/2017-12/competency_framework_for_parkinsons_nurses_2016.pdf (accessed on 29 June 2020).
- Brown, M.T.; Bussell, J.K. Medication adherence: WHO cares? Mayo Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Grosset, D.; Antonini, A.; Canesi, M.; Pezzoli, G.; Lees, A.; Shaw, K.; Cubo, E.; Martinez-Martin, P.; Rascol, O.; Negre-Pages, L.; et al. Adherence to antiparkinson medication in a multicenter European study. Mov. Disord. 2009, 24, 826–832. [Google Scholar] [CrossRef]
- Sabaté, E. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Straka, I.; Minar, M.; Skorvanek, M.; Grofik, M.; Danterova, K.; Benetin, J.; Kurca, E.; Gazova, A.; Bolekova, V.; Wyman-Chick, K.A.; et al. Adherence to Pharmacotherapy in Patients With Parkinson’s Disease Taking Three and More Daily Doses of Medication. Front. Neurol. 2019, 10, 799. [Google Scholar] [CrossRef] [Green Version]
- Valldeoriola, F.; Coronell, C.; Pont, C.; Buongiorno, M.T.; Camara, A.; Gaig, C.; Compta, Y.; ADHESON Study Group. Socio-demographic and clinical factors influencing the adherence to treatment in Parkinson’s disease: The ADHESON study. Eur. J. Neurol. 2011, 18, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.F.; Thirumoorthy, T.; Kwan, Y.H. Systematic review of the barriers affecting medication adherence in older adults. Geriatr. Gerontol. Int. 2016, 16, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Mendorf, S.; Witte, O.W.; Grosskreutz, J.; Zipprich, H.M.; Prell, T. What Predicts Different Kinds of Nonadherent Behavior in Elderly People With Parkinson’s Disease? Front. Med. 2020, 7, 103. [Google Scholar] [CrossRef] [PubMed]
- Bhidayasiri, R.; Boonpang, K.; Jitkritsadakul, O.; Calne, S.M.; Henriksen, T.; Trump, S.; Chaiwong, S.; Chaiwong, S.; Boonrod, N.; Sringean, J.; et al. Understanding the role of the Parkinson’s disease nurse specialist in the delivery of apomorphine therpy. Parkinsonism Relat. Disord. 2016, 33, S49–S55. [Google Scholar] [CrossRef]
- Hagell, P. Nursing and multidisciplinary interventions for Parkinson’s disease: What is the evidence? Parkinsonism Relat. Disord. 2007, 13, S501–S508. [Google Scholar] [CrossRef]
- Mai, T. Status and development of the role as Parkinson Nurse in Germany—An online survey. Pflege 2018, 31, 181–189. [Google Scholar] [CrossRef]
- Reynolds, H.; Wilson-Barnett, J.; Richardson, G. Evaluation of the role of the Parkinson’s disease nurse specialist. Int. J. Nurs. Stud. 2000, 37, 337–349. [Google Scholar] [CrossRef]
- Shin, J.Y.; Hendrix, C.C. Management of patients with Parkinson disease. Nurse Pract. 2013, 38, 34–43. [Google Scholar] [CrossRef]
- Frundt, O.; Mainka, T.; Schonwald, B.; Muller, B.; Dicusar, P.; Gerloff, C.; Buhmann, C. The Hamburg Parkinson day-clinic: A new treatment concept at the border of in- and outpatient care. J. Neural Transm. 2018, 125, 1461–1472. [Google Scholar] [CrossRef]
- Weck, C.E.; Lex, K.M.; Lorenzl, S. Telemedicine in Palliative Care: Implementation of New Technologies to Overcome Structural Challenges in the Care of Neurological Patients. Front. Neurol. 2019, 10, 510. [Google Scholar] [CrossRef]
- Tonges, L.; Ehret, R.; Lorrain, M.; Riederer, P.; Mungersdorf, M. Epidemiology of Parkinson’s Disease and Current Concepts of Outpatient Care in Germany. Fortschr. Neurol. Psychiatr. 2017, 85, 329–335. [Google Scholar]
- Tonges, L.; Bartig, D.; Muhlack, S.; Jost, W.; Gold, R.; Krogias, C. Characteristics and dynamics of inpatient treatment of patients with Parkinson’s disease in Germany: Analysis of 1.5 million patient cases from 2010 to 2015. Der Nervenarzt 2019, 90, 167–174. [Google Scholar]
- Gunther, H.J.; Bader, C.; Erlenberg, R.M.; Hagl, C.; Schirrmacher, B.; Schuster, A. From AGnES to PA-medical assistant professions in Germany: Who still keeps the track? MMW Fortschr. Med. 2019, 161, 21–30. [Google Scholar] [PubMed] [Green Version]
- Mergenthal, K.G.C.; Beyer, M.; Gerlach, F.M.; Siebenhofer, A. Wie bewerten und akzeptieren Patienten die Betreuung durch Medizinische Fachangestellte in der Hausarztpraxis? Ergebnisse einer Patienten-Befragung in der HzV in Baden-Württemberg [How Patients View and Accept Health Care Services Provided by Health Care Assistants in the General Practice: Survey of Participants of the GP-centered Health Care Program in Baden-Wuerttemberg]. Das Gesundh. 2018, 80, 1077–1083. [Google Scholar]
- DBfP (DBfK). Community Health Nursing in Deutschland. Konzeptionelle Ansatzpunkte Für Berufsbild und Curriculum. 2019. Available online: https://www.dbfk.de/media/docs/Bundesverband/CHN-Veroeffentlichung/Broschuere-Community-Health-Nursing-09-2019.pdf (accessed on 29 June 2020).
- Geithner, L.; Doris, A.; Alexandra, F.; Anna, H.; Maike, S.; Tatjana, S. Advanced Nursing Practice: Rahmenbedingungen in Deutschland und Literaturübersicht zu Nationalen und Internationalen Modellen Erweiterter Pflegepraxis. Available online: https://www.e-hoch-b.de/fileadmin/user_upload/Dokumente/Geithner_et_al-2016-ANP.pdf (accessed on 29 June 2020).
- Prell, T.; Siebecker, F.; Lorrain, M.; Eggers, C.; Lorenzl, S.; Klucken, J.; Warnecke, T.; Buhmann, C.; Tonges, L.; Ehret, R.; et al. Recommendations for Standards of Network Care for Patients with Parkinson’s Disease in Germany. J. Clin. Med. 2020, 9, 1455. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.Y.; Habermann, B. Nursing Research in Parkinson’s Disease From 2006 to 2015. Clin. Nurs. Res. 2017, 26, 142–156. [Google Scholar] [CrossRef]


{kind=link}
| Target Group and Prerequisite | Education Curriculum | State Certificate | Setting | Organization | |
|---|---|---|---|---|---|
| Parkinson’s disease specialist nurse | health and nursing professionals minimum of 2 years of professional experience in acute neurological departments or PD hospitals | 4 × 2 days of theoretical training +2 weeks of hospital observation, spread over one year | none | inpatient outpatient | Deutsche Parkinson-Gesellschaft, DPG, Deutsche Parkinsonvereinigung, dPV, Kompetenznetz Parkinson, KNP, Verein der Parkinsonnurses u.–assistenten, VPNA |
| Parkinson assistant | mainly medical assistants with formerly three-year training | basic course (24 teaching hours) advanced course (1-day workshop) | none | inpatient outpatient | QUANUP e. V. |
| Parkinson care specialist | nurse | two days training in PD center | none | inpatient outpatient | Verein der Parkinsonnurses u.–assistenten, VPNA |
| VERAH (Versorgungsassistentin in der Hausarztpraxis) | medical assistant | 200 teaching units + internship of 40 units | yes | outpatient (GP) | Deutscher Hausärzteverband |
| AGnESzwei (Arztentlastende, Gemeindenahe, E-health-gestützte systemische intervention) | nurse or medical assistant | 129 theoretical teaching units | yes | outpatient (GP) | Arbeitsgemeinschaft “Innovative Gesundheitsversorgung in Brandenburg” (IGiB)–der KVBB |
| EVA (Entlastende Versorgungsassistentin) | nurse or medical assistant | at least 300 teaching h | yes | outpatient (GP) | Nordrheinische Akademie |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prell, T.; Siebecker, F.; Lorrain, M.; Tönges, L.; Warnecke, T.; Klucken, J.; Wellach, I.; Buhmann, C.; Wolz, M.; Lorenzl, S.; et al. Specialized Staff for the Care of People with Parkinson’s Disease in Germany: An Overview. J. Clin. Med. 2020, 9, 2581. https://doi.org/10.3390/jcm9082581
Prell T, Siebecker F, Lorrain M, Tönges L, Warnecke T, Klucken J, Wellach I, Buhmann C, Wolz M, Lorenzl S, et al. Specialized Staff for the Care of People with Parkinson’s Disease in Germany: An Overview. Journal of Clinical Medicine. 2020; 9(8):2581. https://doi.org/10.3390/jcm9082581
Chicago/Turabian StylePrell, Tino, Frank Siebecker, Michael Lorrain, Lars Tönges, Tobias Warnecke, Jochen Klucken, Ingmar Wellach, Carsten Buhmann, Martin Wolz, Stefan Lorenzl, and et al. 2020. "Specialized Staff for the Care of People with Parkinson’s Disease in Germany: An Overview" Journal of Clinical Medicine 9, no. 8: 2581. https://doi.org/10.3390/jcm9082581