
Hemodialysis and Peritoneal Dialysis in Germany from a Health Economic View—A Propensity Score Matched Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design & Setting
2.2. Claims Data in the German SHI
3. Study Population
3.1. Identification of Dialysis Modality via EBM Code
3.2. Criteria for Inclusion of Participants
4. Outcomes
4.1. Total Annual Health Care Costs
4.2. Hospitalisations
4.3. Survival
4.4. Charlson Comorbidity Index
4.5. Statistical Analysis
4.6. Propensity Score Matching
4.7. Sensitivity Analysis
5. Results
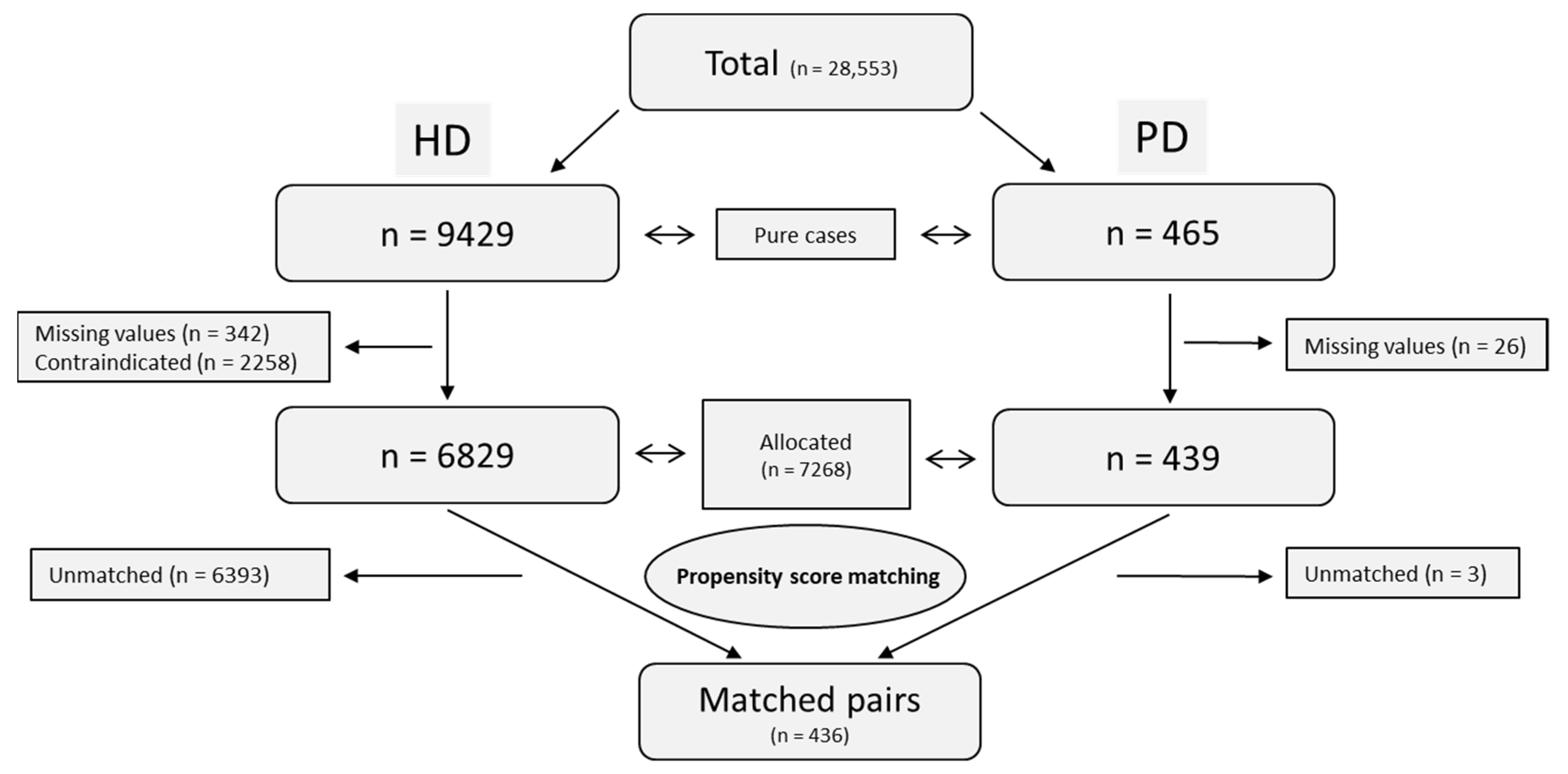
5.1. Propensity Score Analysis and Study Population
5.2. Total Annual Health Care Costs
5.3. Sensitivity Analysis
5.4. Hospitalisations
5.4.1. Hospitalisation Rates
5.4.2. Predictors for Hospitalisations
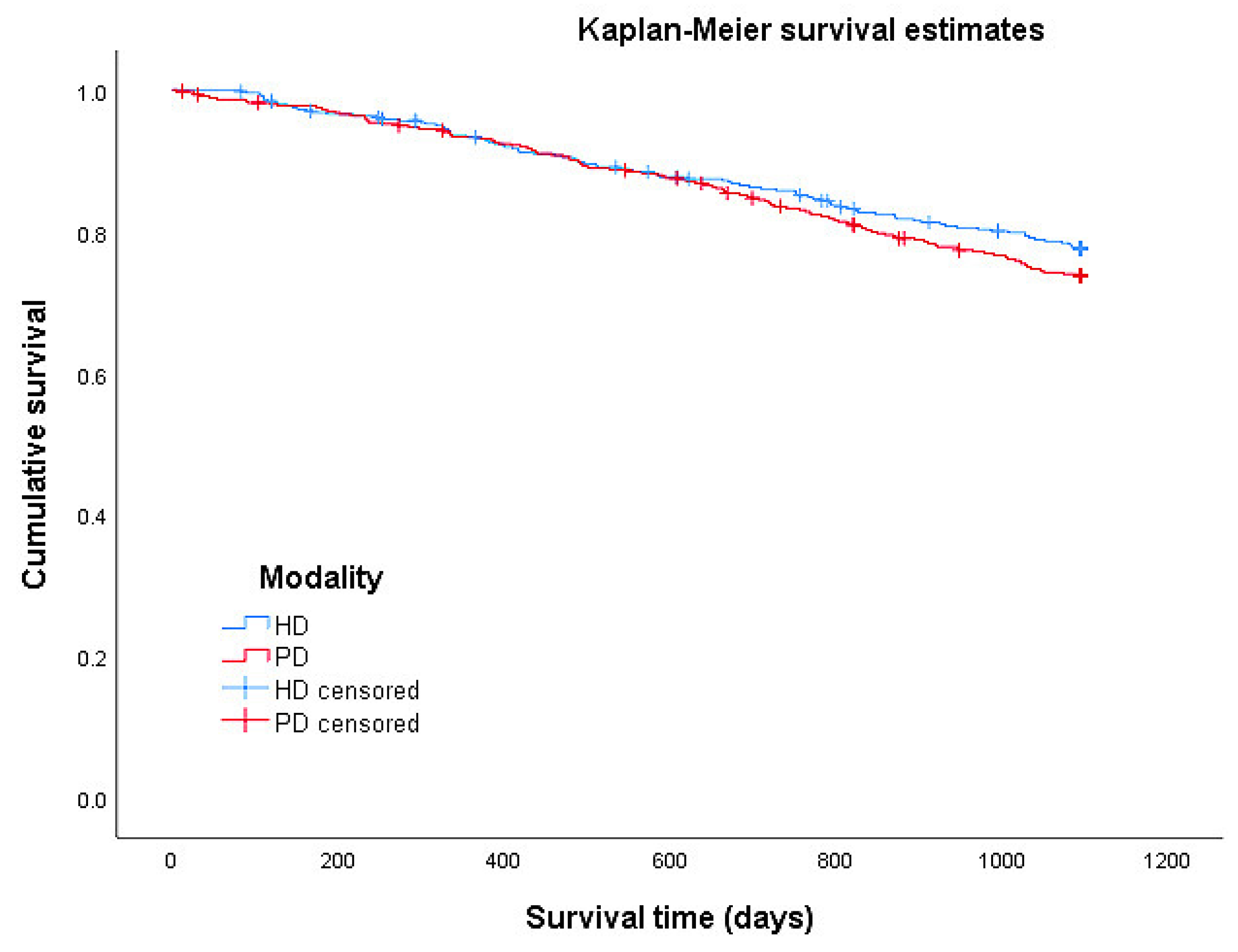
5.5. Survival Analysis
6. Discussion
6.1. Strengths and Limitations
6.2. Future Research
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gandjour, A.; Armsen, W.; Wehmeyer, W.; Multmeier, J.; Tschulena, U. Costs of Patients with Chronic Kidney Disease in Germany. PLoS ONE 2020, 15, e0231375. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, Y.; Higuchi, C.; Io, H.; Wakabayashi, K.; Tsujimoto, H.; Tsujimoto, Y.; Yuasa, H.; Ryuzaki, M.; Ito, Y.; Nakamoto, H. Comparison of Peritoneal Dialysis and Hemodialysis as First Renal Replacement Therapy in Patients with End-Stage Renal Disease and Diabetes: A Systematic Review. Ren. Replace. Ther. 2019, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Sinnakirouchenan, R.; Holley, J.L. Peritoneal Dialysis Versus Hemodialysis: Risks, Benefits, and Access Issues. Adv. Chronic Kidney Dis. 2011, 18, 428–432. [Google Scholar] [CrossRef]
- Wong, B.; Ravani, P.; Oliver, M.J.; Holroyd-Leduc, J.; Venturato, L.; Garg, A.X.; Quinn, R.R. Comparison of Patient Survival between Hemodialysis and Peritoneal Dialysis among Patients Eligible for Both Modalities. Am. J. Kidney Dis. 2018, 71, 344–351. [Google Scholar] [CrossRef]
- Zhou, H.; Sim, J.J.; Bhandari, S.K.; Shaw, S.F.; Shi, J.; Rasgon, S.A.; Kovesdy, C.P.; Kalantar-Zadeh, K.; Kanter, M.H.; Jacobsen, S.J. Early Mortality among Peritoneal Dialysis and Hemodialysis Patients Who Transitioned with an Optimal Outpatient Start. Kidney Int. Rep. 2019, 4, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.-Y.; Jeon, Y.; Park, Y.; Kim, Y.S.; Kang, S.-W.; Yang, C.W.; Kim, N.-H.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; et al. Better Quality of Life of Peritoneal Dialysis Compared to Hemodialysis over a Two-Year Period after Dialysis Initiation. Sci. Rep. 2019, 9, 10266. [Google Scholar] [CrossRef] [Green Version]
- de Fijter, C.W.H.; van Diepen, A.T.N.; Amiri, F.; Dekker, F.W.; Krediet, R.T. Patient-Reported Outcomes (PROs) Argue against the Limited Use of Peritoneal Dialysis in End-Stage Renal Disease. Clin. Nephrol. 2018, 90, 94–101. [Google Scholar] [CrossRef]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of Quality of Life between Patients Underwent Peritoneal Dialysis and Hemodialysis: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Huang, C.-C.; Chang, Y.-C.; Chen, J.-S.; Tsai, W.-C.; Wang, K.-Y. A Comparison of Quality of Life between Patients Treated with Different Dialysis Modalities in Taiwan. PLoS ONE 2020, 15, e0227297. [Google Scholar] [CrossRef]
- Juergensen, E.; Wuerth, D.; Finkelstein, S.H.; Juergensen, P.H.; Bekui, A.; Finkelstein, F.O. Hemodialysis and Peritoneal Dialysis: Patients’ Assessment of Their Satisfaction with Therapy and the Impact of the Therapy on Their Lives. CJASN 2006, 1, 1191–1196. [Google Scholar] [CrossRef]
- Kutner, N.G.; Zhang, R.; Barnhart, H.; Collins, A.J. Health Status and Quality of Life Reported by Incident Patients after 1 Year on Haemodialysis or Peritoneal Dialysis. Nephrol. Dial. Transplant. 2005, 20, 2159–2167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hingwala, J.; Diamond, J.; Tangri, N.; Bueti, J.; Rigatto, C.; Sood, M.M.; Verrelli, M.; Komenda, P. Underutilization of Peritoneal Dialysis: The Role of the Nephrologist’s Referral Pattern. Nephrol. Dial. Transplant. 2013, 28, 732–740. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.K.; Blake, P.; Cordy, P.; Garg, A.X. Global Trends in Rates of Peritoneal Dialysis. J. Am. Soc. Nephrol. 2012, 23, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Choy, A.S.-M.; Li, P.K.-T. Sustainability of the Peritoneal Dialysis-First Policy in Hong Kong. Blood Purif. 2015, 40, 320–325. [Google Scholar] [CrossRef]
- Tennankore, K.K.; Hingwala, J.; Watson, D.; Bargman, J.M.; Chan, C.T. Attitudes and Perceptions of Nephrology Nurses towards Dialysis Modality Selection: A Survey Study. BMC Nephrol. 2013, 14, 192. [Google Scholar] [CrossRef] [Green Version]
- Bouvier, N.; Durand, P.-Y.; Testa, A.; Albert, C.; Planquois, V.; Ryckelynck, J.-P.; Lobbedez, T. Regional Discrepancies in Peritoneal Dialysis Utilization in France: The Role of the Nephrologist’s Opinion about Peritoneal Dialysis. Nephrol. Dial. Transplant. 2008, 24, 1293–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karopadi, A.N.; Mason, G.; Rettore, E.; Ronco, C. Cost of Peritoneal Dialysis and Haemodialysis across the World. Nephrol. Dial. Transplant. 2013, 28, 2553–2569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häckl, D.; Kossack, N.; Schoenfelder, T. Prävalenz, Kosten der Versorgung und Formen des dialysepflichtigen chronischen Nierenversagens in Deutschland: Vergleich der Dialyseversorgung innerhalb und außerhalb stationärer Pflegeeinrichtungen. Gesundheitswesen 2021, 83, 818–828. [Google Scholar] [CrossRef]
- Chang, Y.-T.; Hwang, J.-S.; Hung, S.-Y.; Tsai, M.-S.; Wu, J.-L.; Sung, J.-M.; Wang, J.-D. Cost-Effectiveness of Hemodialysis and Peritoneal Dialysis: A National Cohort Study with 14 Years Follow-up and Matched for Comorbidities and Propensity Score. Sci. Rep. 2016, 6, 30266. [Google Scholar] [CrossRef]
- Moreno Velásquez, I.; Tribaldos Causadias, M.; Valdés, R.; Gómez, B.; Motta, J.; Cuero, C.; Herrera-Ballesteros, V. End-Stage Renal Disease—Financial Costs and Years of Life Lost in Panama: A Cost-Analysis Study. BMJ Open 2019, 9, e027229. [Google Scholar] [CrossRef]
- Treharne, C.; Liu, F.X.; Arici, M.; Crowe, L.; Farooqui, U. Peritoneal Dialysis and In-Centre Haemodialysis: A Cost-Utility Analysis from a UK Payer Perspective. Appl. Health Econ. Health Policy 2014, 12, 409–420. [Google Scholar] [CrossRef] [Green Version]
- Neil, N.; Guest, S.; Wong, L.; Inglese, G.; Bhattacharyya, S.K.; Gehr, T.; Walker, D.R.; Golper, T. The Financial Implications for Medicare of Greater Use of Peritoneal Dialysis. Clin. Ther. 2009, 31, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Davenport, A.; Hannedouche, T.; Kooman, J.; Kribben, A.; Lameire, N.; Lonnemann, G.; Magner, P.; Mendelssohn, D.; Saggi, S.J.; et al. Reimbursement of Dialysis: A Comparison of Seven Countries. J. Am. Soc. Nephrol. 2012, 23, 1291–1298. [Google Scholar] [CrossRef] [Green Version]
- Icks, A.; Haastert, B.; Gandjour, A.; Chernyak, N.; Rathmann, W.; Giani, G.; Rump, L.-C.; Trapp, R.; Koch, M. Costs of Dialysis--A Regional Population-Based Analysis. Nephrol. Dial. Transpl. 2010, 25, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleophas, W.; Reichel, H. International Study of Health Care Organization and Financing: Development of Renal Replacement Therapy in Germany. Int. J. Health Care Financ. Econ. 2007, 7, 185–200. [Google Scholar] [CrossRef]
- DAK. Über Uns. Available online: https://www.Dak.de/Dak/Unternehmen/Ueber-Uns-2091798.Html#/ (accessed on 5 July 2021).
- SBK. Über Uns. Available online: https://www.Sbk.Org/Unternehmen-Sbk/Ueber-Uns/ (accessed on 5 July 2021).
- National Association of Statutory Health Insurance Physicians. Doctor’s Fee Scale: 3rd Quarter 2017. [Einheitlicher Bewertungsmaßstab (EBM): Stand: 3. Quartal 2017]; National Association of Statutory Health Insurance Physicians: Berlin, Germany, 2017. [Google Scholar]
- Schellartz, I.; Mettang, S.; Shukri, A.; Scholten, N.; Pfaff, H.; Mettang, T. Early Referral to Nephrological Care and the Uptake of Peritoneal Dialysis. An Analysis of German Claims Data. Int. J. Environ. Res. Public Health 2021, 18, 8359. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Haastert, B.; Koch, M.; Giani, G.; Glaeske, G.; Icks, A. The Effect of Diabetes on Incidence and Mortality in End-Stage Renal Disease in Germany. Nephrol. Dial. Transplant. 2011, 26, 1634–1640. [Google Scholar] [CrossRef] [Green Version]
- Routinedaten im Gesundheitswesen: Handbuch Sekundärdatenanalyse: Grundlagen, Methoden und Perspektiven; Swart, E.; Ihle, P.; Gothe, H.; Matusiewicz, D. (Eds.) Huber: Bern, Switzerland, 2014; ISBN 978-3-456-85435-9. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.R-project.org (accessed on 16 June 2021).
- Hansen, B.B.; Bowers, J. Covariate Balance in Simple, Stratified and Clustered Comparative Studies. Statist. Sci. 2008, 23, 219–236. [Google Scholar] [CrossRef]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Thoemmes, F. Propensity Score Matching in SPSS. arXiv 2012, arXiv:1201.6385. [Google Scholar]
- Leite, W. Practical Propensity Score Methods Using R; Sage: Los Angeles, CA, USA, 2017; ISBN 978-1-4522-8888-8. [Google Scholar]
- Coreth-Studie. Available online: https://www.Dgfn.Eu/Pressemeldung/Nierenersatztherapie-Coreth-Forschungsprojekt-Liefert-Neue-Erkenntnisse-Zur-Verfahrenswahl.html (accessed on 19 July 2022).
- Voss, P. Modellierung Eines Patientenorientierten Versorgungsoptimums von Niereninsuffizienzpatienten in Deutschland; Schriftenreihe Gesundheitsmanagement und Medizinökonomie; Verlag Dr. Kovač: Hamburg, Germany, 2018; ISBN 978-3-8300-9936-9. [Google Scholar]
- Oliver, M.J.; Al-Jaishi, A.A.; Dixon, S.N.; Perl, J.; Jain, A.K.; Lavoie, S.D.; Nash, D.M.; Paterson, J.M.; Lok, C.E.; Quinn, R.R. Hospitalization Rates for Patients on Assisted Peritoneal Dialysis Compared with In-Center Hemodialysis. CJASN 2016, 11, 1606–1614. [Google Scholar] [CrossRef] [Green Version]
- Banshodani, M.; Kawanishi, H.; Moriishi, M.; Shintaku, S.; Tsuchiya, S. Association between Dialysis Modality and Infectious Diseases: Peritoneal Dialysis versus Hemodialysis. Blood Purif. 2021, 50, 370–379. [Google Scholar] [CrossRef]
- Harris, S.A.C.; Lamping, D.L.; Brown, E.A.; Constantinovici, N. North Thames Dialysis Study (NTDS) Group Clinical Outcomes and Quality of Life in Elderly Patients on Peritoneal Dialysis versus Hemodialysis. Perit. Dial. Int. 2002, 22, 463–470. [Google Scholar]
- Huang, C.-C.; Cheng, K.-F.; Wu, H.-D.I. Survival Analysis: Comparing Peritoneal Dialysis and Hemodialysis in Taiwan. Perit. Dial. Int. 2008, 28 (Suppl. S3), S15–S20. [Google Scholar] [CrossRef] [PubMed]
- MNC Medical Netcare GmbH. Annual Report about the Quality in Dialysis 2016 [Jahresbericht 2016 zur Qualität in der Dialyse]; MNC Medical Netcare GmbH: Münster, Germany, 2017; p. 59. [Google Scholar]



{kind=link}
{kind=link}
| Before Matching | After Matching | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HD (n = 6829) | PD (n = 439) | HD (n = 436) | PD (n = 436) | ||||||||
| n | % | n | % | p-Value | n | % | n | % | p-Value | ||
| Sex | Women | 2860 | 41.9 | 181 | 41.2 | 0.789 | 178 | 40.8 | 178 | 40.8 | 1.000 |
| Men | 3969 | 58.1 | 258 | 58.8 | 258 | 59.2 | 258 | 59.2 | |||
| Age | 18–44 years | 392 | 5.7 | 71 | 16.2 | 0.000 | 68 | 15.6 | 68 | 15.6 | 1.000 |
| 45–64 years | 1850 | 27.1 | 197 | 44.9 | 197 | 45.2 | 197 | 45.2 | |||
| 65–74 years | 2032 | 29.8 | 108 | 24.6 | 108 | 24.8 | 108 | 24.8 | |||
| 74–84 years | 2041 | 29.9 | 57 | 13.0 | 57 | 13.1 | 57 | 13.1 | |||
| ≥85 years | 514 | 7.5 | 6 | 1.4 | 6 | 1.4 | 6 | 1.4 | |||
| Region | North | 1498 | 21.9 | 66 | 15.0 | 0.001 | 65 | 14.9 | 65 | 14.9 | 1.000 |
| East | 1105 | 16.2 | 65 | 14.8 | 64 | 14.7 | 64 | 14.7 | |||
| South | 2019 | 29.6 | 137 | 31.2 | 137 | 31.4 | 137 | 31.4 | |||
| West | 2207 | 32.3 | 171 | 39.0 | 170 | 39.0 | 170 | 39.0 | |||
| Age Mean (SD) | 68.5 (13.2) | 59.3 (14.4) | 0.000 | 59.8 (14.2) | 59.4 (14.6) | 0.747 | |||||
| CCI Mean (SD) | 6.7 (3.5) | 5.4 (3.3) | 0.000 | 5.4 (3.2) | 5.4 (3.3) | 1.000 | |||||
| Cost Types | HD | PD | HD-PD a | 95% CI * | p-Value |
|---|---|---|---|---|---|
| Total | 47,501 | 46,235 | 1266 | −2879–5487 | 0.557 |
| Outpatient services 1 | 24,158 | 23,335 | 823 | −864–2413 | 0.336 |
| Drug expenses | 8144 | 5961 | 2183 | 736–3614 | 0.003 |
| Sick pay | 304 | 575 | −271 | −544–−3 | 0.048 |
| Therapeutic aids | 602 | 423 | 179 | 2–341 | 0.043 |
| Inpatient services 1 | 13,974 | 15,799 | −1825 | −5545–1832 | 0.317 |
| Rehabilitation | 319 | 143 | 176 | 36–328 | 0.017 |
| Total | Event | Censored | Survival in Days | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | Estimator | SE | 95% CI | ||
| HD | 436 | 95 | 21.8 | 341 | 78.2 | 977.5 | 12.6 | 952.8–1002.2 |
| PD | 436 | 112 | 25.7 | 324 | 74.3 | 963.3 | 13.0 | 937.9–988.7 |
| Total | 872 | 207 | 23.7 | 665 | 76.3 | 970.4 | 9.0 | 952.7–988.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shukri, A.; Mettang, T.; Scheckel, B.; Schellartz, I.; Simic, D.; Scholten, N.; Müller, M.; Stock, S. Hemodialysis and Peritoneal Dialysis in Germany from a Health Economic View—A Propensity Score Matched Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14007. https://doi.org/10.3390/ijerph192114007
Shukri A, Mettang T, Scheckel B, Schellartz I, Simic D, Scholten N, Müller M, Stock S. Hemodialysis and Peritoneal Dialysis in Germany from a Health Economic View—A Propensity Score Matched Analysis. International Journal of Environmental Research and Public Health. 2022; 19(21):14007. https://doi.org/10.3390/ijerph192114007
Chicago/Turabian StyleShukri, Arim, Thomas Mettang, Benjamin Scheckel, Isabell Schellartz, Dusan Simic, Nadine Scholten, Martin Müller, and Stephanie Stock. 2022. "Hemodialysis and Peritoneal Dialysis in Germany from a Health Economic View—A Propensity Score Matched Analysis" International Journal of Environmental Research and Public Health 19, no. 21: 14007. https://doi.org/10.3390/ijerph192114007