
Statistical Insight into China’s Indigenous Diagnosis-Related-Group System Evolution
by
Wenlong Ma
1,
Jing Qu
2,
Hui Han
3,
Zixia Jiang
4,
Tiantian Chen
2,
Xuefeng Lu
1 and
Jiaoyang Lu
1,5,* 1
Department of Gastroenterology, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan 250012, China
2
Department of Medical Records, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan 250012, China
3
Office of Hospital President, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan 250012, China
4
Department of Medical Insurance, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan 250012, China
5
Medical Integration and Practice Center, Cheeloo College of Medicine, Shandong University, Jinan 250012, China
*
Author to whom correspondence should be addressed.
Healthcare 2023, 11(22), 2965; https://doi.org/10.3390/healthcare11222965
Submission received: 17 September 2023
/
Revised: 9 November 2023
/
Accepted: 12 November 2023
/
Published: 15 November 2023
(This article belongs to the Section Health Policy)
Abstract
:The use of Diagnosis-Related Groups (DRG) is a prevalent payment system employed to control hospitalization costs and improve medical efficiency. China has developed an indigenized DRG payment system including Single Disease Payment (SDP), DRGs, and Big Data Diagnosis-Intervention Packet (DIP). In this study, we took cholecystitis as an example, drawing on both primary and secondary data to verify the effectiveness of China’s indigenized DRG system and to introduce the evolution of DRGs in China. Primary data were gathered from Qilu Hospital in 2019–2021. Secondary data were collected from published literature from 2004–2016. Only studies with both pre-SDP/DRG and post-SDP/DRG groups were included. Among the studies included, 92.9% (13/14) reported a significant reduction in hospitalization costs after the implementation of SDP while other studies identified length of stay (LOS) and age as the most significant influential factors in SDP. Furthermore, we elaborated the efficiency of DRGs using data from 2738 inpatients in Qilu hospital. Moreover, 60% (6/10) of the studies from the databases also showed the efficiency of DRGs in different regions. SDP is efficient in saving hospitalization costs, but its implementation is limited. DRGs have a broader scope of application, but their effectiveness remains to be validated. DIP is a brand new concept in China, and more data are needed to assess its efficiency.
1. Introduction
Originating at Yale University, Diagnosis-Related Groups (DRGs) were first implemented in the United States in 1983 and are considered a highly effective payment system to improve efficiency, including controlling hospitalization costs and increasing medical efficiency. In this payment system, patients are classified into groups based on their diagnosis and additional characteristics, such as age, complications, and operations, allowing medical expenses to be directly related to the group [1]. Over the past three decades, DRGs have been widely adopted and utilized by several developed countries, including the United States, Australia, Finland, France, Germany, and Japan [2,3,4,5]. Taking Japan, an Asian country, as an example, Hamada et al. evaluated the impact of the diagnostic procedure combination/per-diem payment system (DPC/PDPS) (known as the Japanese DRGs) and discovered that this system could decrease medical expenses. This was evidenced by a decrease in both the average per capita hospitalization cost and the length of stay (LOS) in hospitals [2].
As the world’s most populous developing country, China has made significant progress in providing Universal Health Coverage through three independent insurance systems that cover employed workers, city residents, and farmers, accounting for over 95% of the population [6]. However, this progress has resulted in high health expenditures and has put pressure on the limited national insurance funding in recent years. In response, the Chinese government has been searching for an alternative payment system that can provide essential healthcare services to the majority of the population while reducing spending, and DRG has emerged as a potential solution.
Taking China’s national conditions into consideration, the Chinese government has successively developed a system including three kinds of indigenous DRGs: Single-Disease Payment (SDP, which is also regarded as simplified DRG), DRG, and the recent Big Data Diagnosis-Intervention Packet (DIP). The interplay among SDP, DRG, and DIP can be likened to an intricate trio in the realm of healthcare reform: SDP serves as a succinct yet indispensable component, initiating the prelude of China’s healthcare reform; DRG assumes the role of a classic melody, propelling reform efforts forward; and DIP incorporates ethnic elements to create a harmonious resolution, offering a uniquely Chinese approach. Together, these three components intertwine and reinforce each other, producing a resounding crescendo in China’s ongoing medical reform narrative.
Though this system is marvelous, previous studies only investigated the effect of SDP [7] or DRG [8] alone, but failed to uncover the intrinsic connection between them, nor distinguished their respective roles in reducing cost and increasing medical efficiency. In this study, we took cholecystitis, a common disease of the digestive system, as an example to elaborate the evolution and differentiation of the three indigenous DRGs. Additionally, we analyzed recent studies to determine the effectiveness of these DRGs in reducing expenditures and improving medical efficiency. By providing an overview of the development of DRGs in China and evaluating their benefits and drawbacks at each stage, we aimed to offer insights into building a high-efficiency, cost-effective Universal Public Insurance system in China and other developing countries.
2. Materials and Methods
This study utilized both primary and secondary data sources to assess the effectiveness of China’s characteristic DRGs in reducing medical expenses and increasing medical efficiency in hospitals.
2.1. Primary Data Collection
Primary data were gathered from Qilu Hospital, a large regional medical center located in a province with a population of over 100 million people. DRG was integrated into the hospital information system on 1 October 2019 and was put into trial operation on 30 September 2020. Based on this timeline, patients with cholecystitis-related disorders admitted to Qilu Hospital between 1 October 2019 to 30 September 2021 were divided into a “pre-DRG” group and a “post-DRG” group. Cholecystitis-related disorders were identified using the primary diagnosis with the International Classification of Diseases, 9th Revision, Clinical Modification of Operations and Procedures, ICD-9-CM-3. The study population included 2738 patients with cholecystitis-related disorders, which were stratified into two groups based on their index data (N = 1172 before the DRG from 1 October 2019 to 30 September 2020; and N = 1566 after the DRG from 1 October 2020 to 30 September 2021). All costs were analyzed based on charge reports from the hospital.
2.2. Secondary Data from Published Literature
2.2.1. Search Strategy and Selection Criteria
A comprehensive literature search was conducted in electronic databases including Scopus, PubMed, Web of Science, China National Knowledge Infrastructure Database (CNKI), and Wan Fang Database. The search was conducted using the keywords “Diagnosis-Related Groups” [Mesh], “Single Disease Payment,” “Diagnosis-Intervention Packet (DIP),” “Cholecystitis” [Mesh], and “China” [Mesh], and was limited to articles published between 2004 and September 2022. The beginning year of 2004 was selected because it marked the nationwide implementation of the Single-Disease Payment (SDP) in China. In the assessment of DRG efficiency, the search was further limited to articles published between 2019 and September 2022 following a prior systematic review [8].
2.2.2. Data Extraction
Data extraction was performed by one reviewer (Wenlong Ma) and was independently verified by another reviewer (Jiaoyang Lu). Any discrepancies were resolved through discussion. The extracted data for evaluating the efficiency of SDP and DRG included the first author, publication year, study location, number of pre-SDP/DRG groups, number of post-SDP/DRG groups, length of stay (LOS), and total expenditure (TE). To evaluate the factors affecting the hospitalization cost of cholecystitis, data on the first author, publication year, and logistic regression indicators including length of stay, complications, age, gender, and operation were extracted.
3. Results
3.1. Study Selection
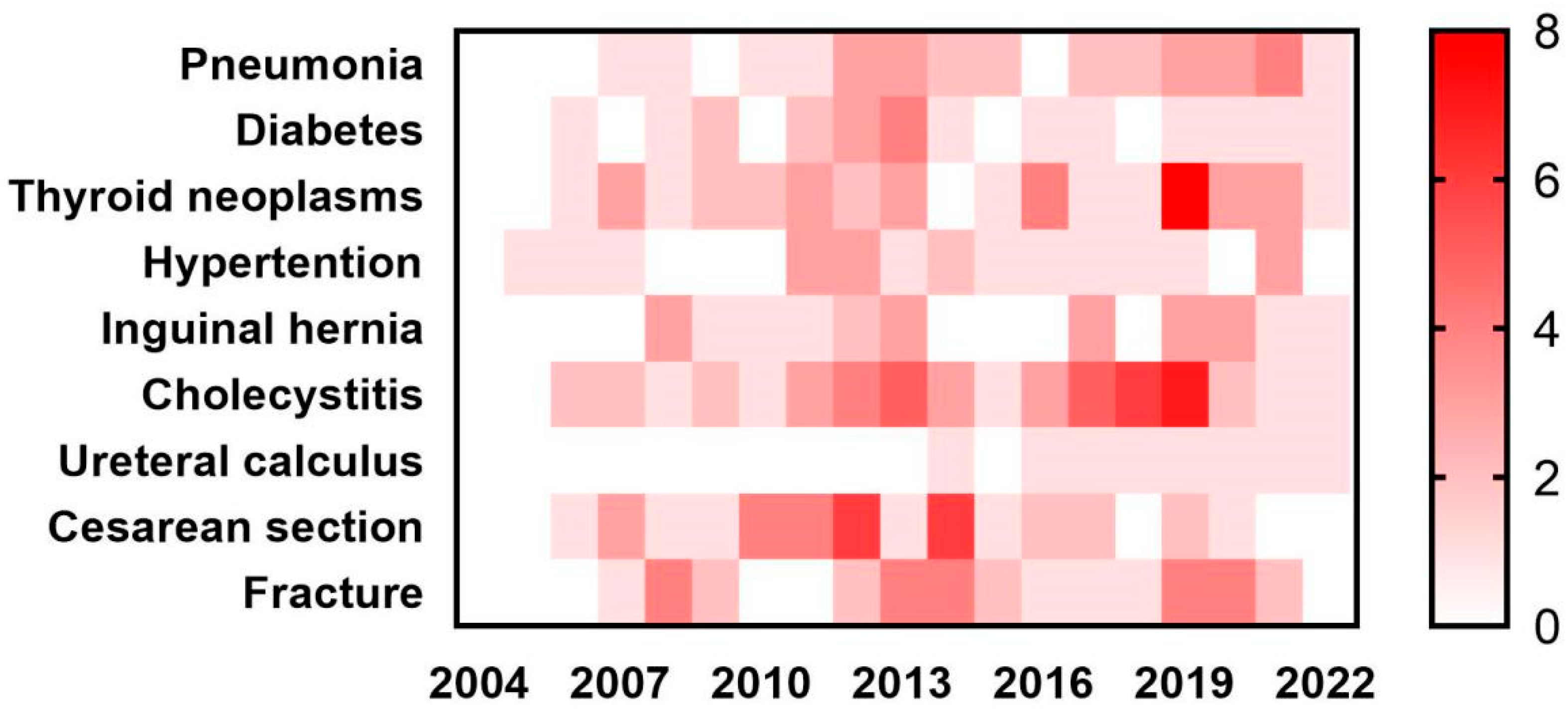
We initially conducted a literature review of studies examining the efficiency of SDP system for various common diseases, including pneumonia, diabetes, thyroid neoplasms, hypertension, inguinal hernia, cholecystitis, ureteral calculus, cesarean section, and fracture (Figure 1). A heat map was generated based on the results of 254 studies. Given the large sample size and diverse characteristics of the diseases studied, cholecystitis was selected as the focus of our further analysis.
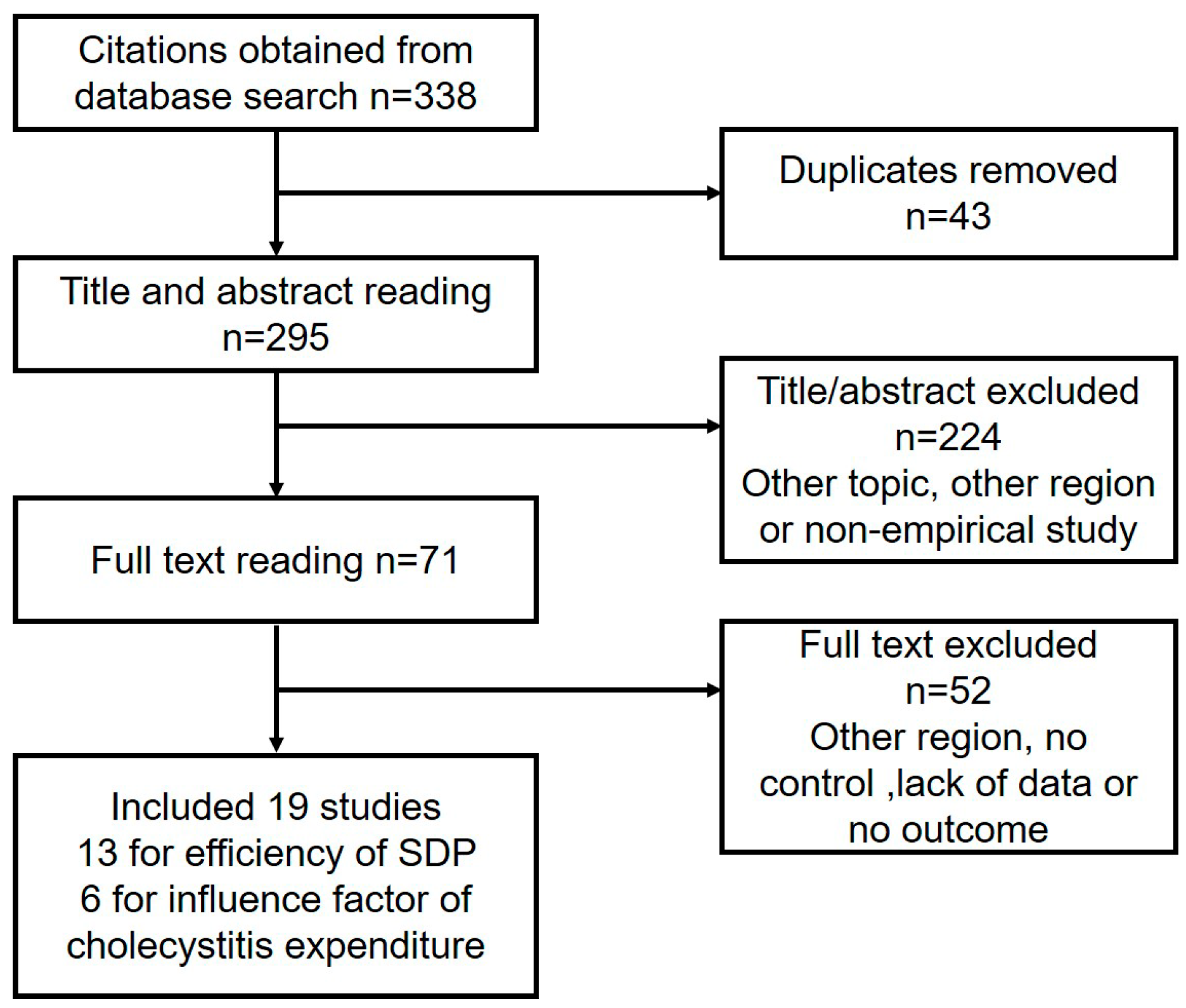
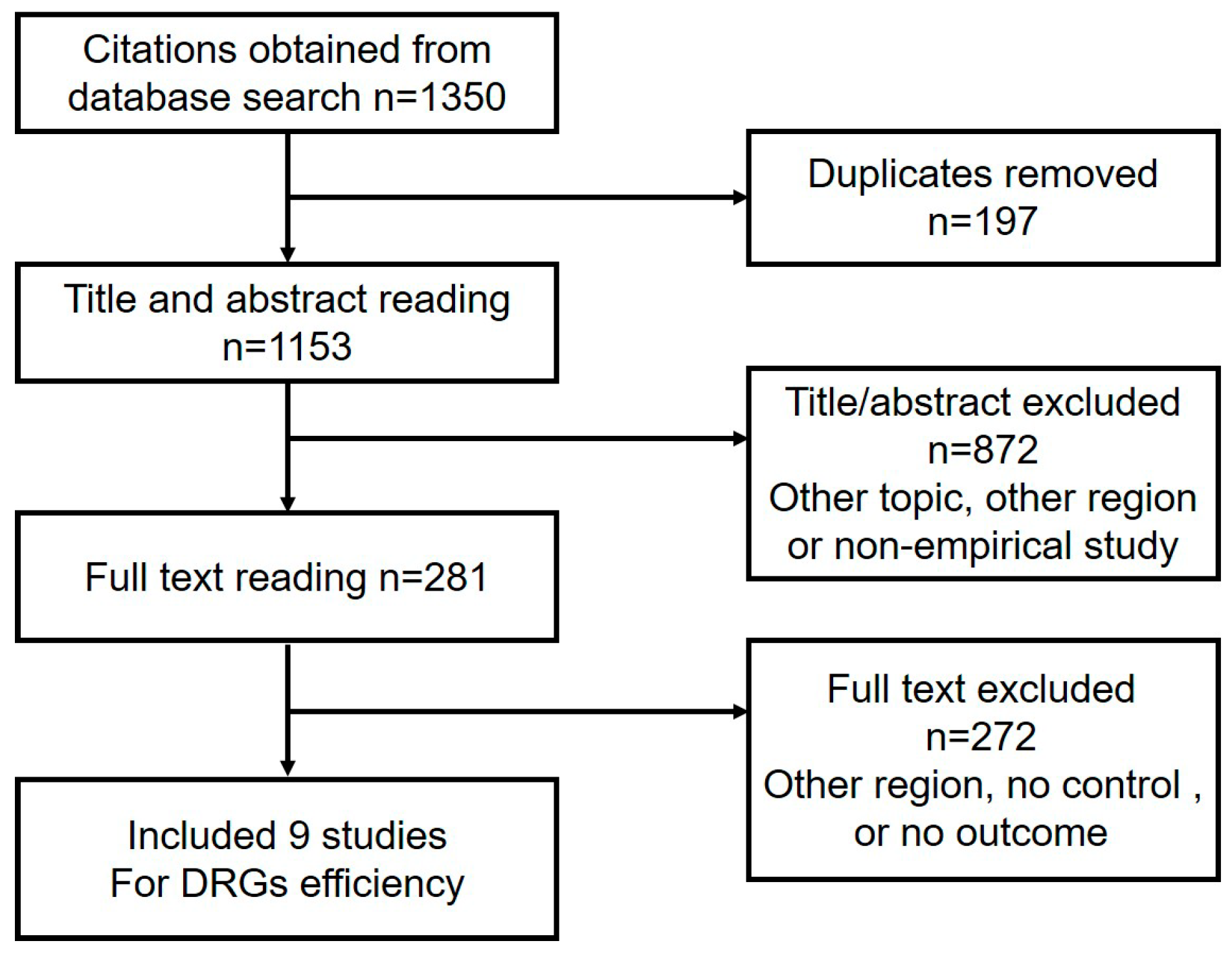
In total, 338 studies were identified that investigated either the impact of the SDP or the factors influencing the cost of treating cholecystitis. After eliminating duplicates, we reviewed the titles and abstracts of 295 articles and excluded 224 of them due to their irrelevant topics, regions, or lack of empirical studies. We then thoroughly read the full text of the remaining 71 citations and finally included 19 publications (13 studies on SDP and 6 studies on the factors influencing cost) in our analysis (Figure 2). Furthermore, from the original search results of 1350 studies, we selected 9 studies for further analysis of the efficiency of DRG (Figure 3).
Among the nine studies evaluated for efficiency of DRG, two were conducted in Guangdong and one each in Henan, Yunnan, Beijing, Zhejiang, Liaoning, Hubei, and Sichuan. All studies included pre-DRG and post-DRG groups. All of them compared the total expenditure, and eight studies included data of LOS (Figure 3).
3.2. Characteristics of the Included Publications
The 19 SDP studies included were conducted in different areas of China: three in Shandong, two each in Yunnan, Hunan, Anhui, Jiangsu, Jilin, Hubei, and Beijing, and one each in Liaoning and Tianjin. All studies for efficiency of SDP included post-SDP group (implementing SDP) and pre-SDP group (traditional payment system, not implementing SDP). Fourteen studies reporting total expenditure and LOS were used for evaluating the efficiency of SDP; six studies using logistic regression to predict potential influencing factors such as LOS, complication, age, gender, and operation were pooled and analyzed.
3.3. Efficiency of SDP
The implementation of the SDP resulted in a significant reduction in the total expenditure for treating cholecystitis in 92.9% (13/14) of the studies [9,10,11,12,13,14,15,16,17,18,19,20,21], with a maximum reduction of half [13,21]. This demonstrated that SDP was effective in controlling cost (Table 1). However, the cost of treating cholecystitis without surgery was not significantly reduced after the implementation of SDP in some studies [17], suggesting that surgical instruments and consumables are the primary target for cost control, rather than examinations or medications.
The cost of laparoscopic cholecystectomy varied significantly between regions and hospitals, ranging from 5000 to 20,000 RMB, which may be related to regional development and hospital level. For example, patients treated at tertiary hospitals may incur higher expenses for laparoscopic cholecystectomy due to the presence of more comorbidities and the need for more medical treatment during the perioperative period.
In conclusion, while the SDP is simple and effective in controlling costs for certain cases, it does not account for all potential influencing factors of hospitalization expenses for cholecystitis. Further analysis of these factors is needed to fully understand the cost-saving impact of the SDP (Table 2).
3.4. Factors Influencing Cholecystitis Expense in SDP
Of the six studies included, all recognized LOS and age as having significant impact on hospitalization cost. Interestingly, four studies found gender to be a factor influencing the total cost, with the cost for male patients being significantly higher than that for female patients [22,23,24,25,26]. One possible explanation is that male inpatients tend to be older and have more underlying diseases, surgical history, and complications compared to female inpatients [27]. Moreover, four studies indicated that patients with operations and complications usually tend to incur higher hospitalization costs (Table 2).

{kind=link}
{kind=link}
{kind=link}
Table 2.
Influencing factors of cholecystitis expense in SDP.
| First Author | Province | LOS | Complication | Age | Gender | Operation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | β′ | Sig | β | β′ | Sig | β | β′ | Sig | β | β′ | Sig | β | β′ | Sig | ||
| Jiang (2019) [28] | Shandong | 5.560 | 0.000 | 0.089 | 0.047 | 0.195 | 0.030 | −4.655 | 0.000 | |||||||
| He (2015) [26] | Yunnan | 0.109 | 0.289 | 0.000 | 0.031 | 0.076 | 0.001 | 0.023 | 0.055 | 0.006 | 0.001 | 0.073 | 0.001 | −0.290 | −0.294 | 0.000 |
| Gu (2013) [24] | Tianjin | 0.011 | 0.373 | <0.001 | 0.024 | 0.034 | 0.040 | 0.002 | 0.097 | <0.001 | 0.019 | 0.037 | 0.030 | −0.285 | −0.544 | <0.001 |
| Feng (2010) [23] | Beijing | 1.720 | 0.392 | 0.000 | 0.906 | 0.092 | 0.000 | 0.028 | 0.164 | 0.000 | 0.101 | 0.008 | 0.001 | 1.255 | 0.123 | 0.000 |
| Chen (2006) [22] | Beijing | 0.001 | 0.431 | 0.000 | 0.000 | 0.062 | 0.000 | 0.001 | 0.062 | 0.000 | ||||||
| Guo (2004) [25] | Anhui | 1.853 | 0.310 | 0.000 | 0.080 | 0.084 | 0.050 | 3.460 | 0.122 | 0.004 | ||||||
β, the regression coefficient, reflects the impact degree of expense. β′, the standard regression coefficient, reflects the impact degree of expense without unit influence. A positive value indicates a positive correlation between the factor and hospitalization expenses, while a negative number indicates a negative correlation between the factor and hospitalization expenses. The larger the absolute value, the greater the impact of the factor on hospitalization expenses. Sig, Significance. Female was assigned a value of 1 and male was assigned a value of 2.
3.5. The Way of DRG Grouping Cholecystitis
In light of the factors that influence the cost of cholecystitis treatment under SDP, DRG grouping provided a comprehensive framework for reimbursing cholecystitis treatment. Combined with the above conclusions and practical factors, the current DRG uses the occurrence of complications and surgical methods as the basis for grouping cholecystitis. Cases with severe complications or complex surgery are assigned higher relative weight (RW) values, as demonstrated in Table 3, which includes the number of cases treated in 2020 at Qilu Hospital. The majority of patients fall under the category of “laparoscopic cholecystectomy without common bile duct exploration”, which is equivalent to the “laparoscopic cholecystectomy” category in the SDP system. However, when patients required intensive care or novel technology, these cases were assigned a higher RW value and therefore a higher reimbursement amount. In conclusion, DRG is a more nuanced payment system that takes into account all aspects of medical practice compared to the simple SDP system.
3.6. The Efficiency of DRG in Cholecystitis-Related Disorders
In this study, the impact of DRG was evaluated in the surgical department of Qilu Hospital in the treatment of cholecystitis-related disorders. The results showed that among the 16 disorders included, the total expenditure was positively correlated with LOS. Following the implementation of DRG, 11 of the disorders showed a decrease in both LOS and expenditure, while nine showed an increase. The DRG had a significant impact on reducing both LOS and expenditure in groups with lower Relative Weight (RW) values; however, the effect was less remarkable in groups with higher RW values. This may be due to the fact that patients in groups with higher RW are more likely to have underlying diseases and complications, which can skew the results when the sample population is limited (Table 4).
3.7. Efficiency of DRG
Among the ten results from nine studies, six showed that the post-DRG group spent less than the pre-DRG group [29,30,31,32,33,34], while four demonstrated a completely opposite outcome [30,35,36,37]. One possible explanation for this discrepancy is the difficulty in controlling for cost-influencing factors when selecting samples in DRG due to their complex nature. This can lead to significant differences in variables such as diseases, age, gender, operations, complications, and others between the pre-DRG and post-DRG groups [30,36,37]. However, two studies reversed their results showing that DRG could reduce hospitalization cost significantly after analyzing influencing factors of expenditure with univariate linear regressions and multilevel mixed effects models with robust standard errors [30,36]. Therefore, multiple statistical methods might be necessary to elucidate the role of DRG in reducing expenditures from other confounding factors. Meanwhile, seven articles proposed that DRG could reduce LOS remarkably (Table 5).
4. Discussion
Since the 1980s, China has been exploring the indigenization of DRGs and learning from advanced DRG experience in developed countries. The “Notice on piloting the single disease payment” issued by the Chinese Ministry of Health in November 2004 is regarded as the initial sign of China’s exploration to indigenize DRG [38]. In contract with mature DRG, SDP, which is essentially a prospective payment system, is regarded as a simplified version of DRG. The essence of SDP is that the charge of a medical institution is only related to the diagnosis of a specific disease, but not related to the actual cost to treat the case, the so-called “ceiling price for a single disease” [39].
Our study, taking cholecystitis as an example, found that the implementation of SDP significantly reduced the expenditure and length of hospital stay for cholecystitis. Moreover, three publications reported that patients were satisfied with the SDP system [12,19,20]. and one study reported that SDP raised medical efficiency by increasing inpatient turnover [14]. The results of the analysis of the factors influencing cholecystitis expense in SDP also showed the relevance of expenditure with LOS, gender, age, complications, and operations, which provided a powerful basis for the criteria for subsequent grouping of DRG.
However, as defined, SDP is just a simplified and transitional version of DRG, not a genuine DRG system. The limitations of SDP are evident: its coverage of disease spectrums is limited, it ignores other important factors such as the severity of disease, age, gender, and complications, and it is only concerned with the first diagnosis, with no uniform standards [40,41]. Hence, further innovation and development are needed for a localized DRG system.
In 2008, the Beijing Medical Insurance Association developed the Beijing version of DRG (BJ-DRG), which was the first genuine localized DRG system. Since then, various DRG systems have been piloted in different provinces. Currently, there are four widely used and influential DRG systems in China, each with its own features. The BJ-DRG primarily focuses on cost control, CN-DRG emphasizes medical performance evaluation and quality supervision, C-DRG groups diseases innovatively based on the full spectrum, and CHS-DRG is a culmination of all the versions (Table 6).
In this study, average hospitalization cost is remarkably reduced after the implementation of DRG in most research. At the same time, there is no significant difference between the post-DRG group and the pre-DRG group in healthcare quality and safety [30,31,32,33,34,35,36,37]. This finding suggests that DRG can reduce medical costs without affecting medical quality and safety. Two studies also show that patient satisfaction was significantly improved after implementing DRG [30,35]. However, in one study, the low-risk-mortality was higher in the post-DRG group (0.24%) than in the pre-DRG group (0.08%) [30]. In addition, several researchers proposed that some medical institutions have insufficient compensation due to the large number of critically ill patients, which may be the consequence of higher mortality in DRG group [30,33,37]. Moreover, two studies utilizing Data Envelopment Analysis (DEA) revealed that DRG was not effective enough in improving medical efficiency, especially in clinical departments [42,43]. At the same time, DRG relies on high-quality medical records but paradoxically lacks universal standards, making it arduous to popularize in hospitals lacking medical resources.
In order to overcome the regional differences and difficulties in the application of DRG, a new payment convenient to apply in urban hospitals is urgent. Combining the characteristics of big data and traditional DRG, in 2020, the Chinese National Healthcare Security Administration creatively proposed the concept of DIP [44]. Compared with DRG, DIP takes advantage of Big Data to divide different diseases with different surgeries into different groups, which means there is only one disease with or without one specific operation in one group (Table 7). This alteration makes high-quality medical records no longer necessary in payment and enables DIP implementation in remote hospitals lacking healthcare resources.
However, there were several limitations in this study. Firstly, some unpublished studies may have been missed despite identifying and including the largest number of studies. Secondly, although the utilization of DEA provided a more comprehensive perspective for studying the impact of DRG on medical efficiency, the lack of available data affected the accuracy of the results. Thirdly, the details of the components of DRG payment policy and related context were underreported in the included studies, which might limit the interpretation and application of research findings. Lastly, as DIP is a newly proposed concept, there is currently a scarcity of research that evaluates its efficiency. Future studies should focus on collecting relevant data in these areas.
5. Conclusions
At present, the implementation of SDP, DRG, and DIP has spread across both urban and rural areas in all provinces and municipalities in China. These systems are different stages of the indigenization of DRG and complement each other. SDP provides a convenient payment system to control certain disease expenses. DRG, proven effective in many developed countries, displays its potent ability to manage medical costs but is limited in less-developed regions. DIP provides a new method of reducing medical insurance costs by adapting to DRG localization based on the national conditions of developing countries in China, although its efficiency has not yet been evaluated. At different times, each of these three DRG systems fulfills a distinct role and contributes significantly to the achievement of medical cost containment. For developing countries, replicating the DRG system used in developed countries can be challenging due to limited primary care resources. However, the experience of multiple DRG variants complementing each other in China provides a valuable experience in controlling medical expenditure.
Author Contributions
Conceptualization, J.L. and W.M.; methodology, W.M.; software, W.M.; validation, W.M. and J.L.; resources, J.Q., W.M. and T.C.; data curation, J.L. and W.M.; writing—original draft preparation, W.M.; writing—review and editing, J.L.; visualization, J.L.; supervision, J.Q., H.H., Z.J., T.C., X.L. and J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Micro Major Program of Shandong University (qlyxjy-202332) and the Cheeloo Medical Characteristic Undergraduate Education and Teaching Research Project of Shandong University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are not available due to hospital privacy policies.
Acknowledgments
The authors sincerely appreciate Qilu Hospital for data support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jian, W.; Lu, M.; Chan, K.Y.; Poon, A.N.; Han, W.; Hu, M.; Yip, W. Payment Reform Pilot In Beijing Hospitals Reduced Expenditures And Out-Of-Pocket Payments Per Admission. Health Aff. 2015, 34, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Hamada, H.; Sekimoto, M.; Imanaka, Y. Effects of the per diem prospective payment system with DRG-like grouping system (DPC/PDPS) on resource usage and healthcare quality in Japan. Health Policy 2012, 107, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Klein-Hitpass, U.; Scheller-Kreinsen, D. Policy trends and reforms in the German DRG-based hospital payment system. Health Policy 2015, 119, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Mikkola, H.; Keskimaki, I.; Hakkinen, U. DRG-related prices applied in a public health care system—Can Finland learn from Norway and Sweden? Health Policy 2002, 59, 37–51. [Google Scholar] [CrossRef]
- Or, Z. Implementation of DRG Payment in France: Issues and recent developments. Health Policy 2014, 117, 146–150. [Google Scholar] [CrossRef]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Zhao, C.; Wang, C.; Shen, C.; Wang, Q. Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci. Trends 2018, 12, 109–115. [Google Scholar] [CrossRef]
- Huang, G. Recent developments and future trends in China’s urban social security. J. Chin. Gov. 2020, 5, 374–389. [Google Scholar] [CrossRef]
- Tang, X. Influence of Fee for Single Disease Reform on Hospitalization Expenses; Qingdao University: Qingdao, China, 2019. [Google Scholar]
- Chen, Y. The Study on Hospital Expenses of Patients with Cholecystitis Related to DRGs in Anhui Province; Anhui Medical University: Hefei, China, 2016. [Google Scholar]
- Sun, J.; Jiang, J.; Gu, X.; Gu, X. Application of clinical pathway of single-disease in dual referral mechanism of rural elderly patients with gallstone. China Med. Her. 2015, 12, 145–147. [Google Scholar]
- Sun, P. Analysis of the Structure and Influencing Factors of Single Disease Hospitalization Costs in a Tertiary Hospital Based on Clinical Pathway; University of South China: Hengyang, China, 2019. [Google Scholar]
- Wang, M. The Evaluation Study on the Effect of the Clinical Pathway-Based Cost Control of Single Disease—A Research Based on the Cost Control Policy in the Affiliated Hospital of Jining Medical College; Qingdao University: Qingdao, China, 2013. [Google Scholar]
- Kong, X.; Cui, X.; Pan, J.; Shao, H.; Xu, H.; Li, S. The Research on the Application of Clinical Pathways to Limit the Prices of Single Disease Medical Treatment. Jiangsu Health Syst. Manag. 2011, 22, 73–75. [Google Scholar]
- Yu, J. Analysis of Hospital Costs Structure and Influencing Factors of Three Kinds of Single Diseases at a Three Level of First-Class Hospital under Clinical Pathway; Jilin University: Changchun, China, 2012. [Google Scholar]
- Zhang, Y. The Researchof Effect on Control over Single-Disease Charge in Medical Insurance of Onegrade—A Tertiary Hospital in Shenyang; China Medical University: Shenyang, China, 2018. [Google Scholar]
- Zhou, C. The impact of DRGs payment on drug costs in five disease groups of our hospital. Academy 2018, 11, 54–56. [Google Scholar]
- Jiang, S.; Zhang, C. An Analysis of Effect of DRG in Laparoscopic Cholecystectomy of NCMS. Med. Soc. 2009, 22, 23–24+27. [Google Scholar]
- Liu, Y.; Sun, W.; Tao, N. Application research on construction and promotion of clinical pathway platform for nursing management of single disease in surgery. Jilin Med. J. 2009, 30, 557–558. [Google Scholar]
- Ren, A.; Shang, P.; Zhu, X.; Li, Y. The application of the clinical pathway in laparoscopic cholecystectomy limited price management. J. Nurs. Adm. 2007, 2, 45–46,48. [Google Scholar]
- Su, Y. Study on Growth and Trend of Hospitalization Expense of Four Diseases under Different Payment in Changsha Medical Insurance; Central South University: Changsha, China, 2011. [Google Scholar]
- Chen, Y. Research on Analysis of and Control over Influencing Factors of Single Disease’s Hospitalization Expenses in Polyclinic; Army Medical University: Chongqing, China, 2006. [Google Scholar]
- Feng, D.; Liu, J.; Duan, L.; Liu, L. Factors on Direct Cost of Inpatient with Gall-stone Disease. Hosp. Adm. J. Chin. People’s Lib. Army 2010, 17, 530–532. [Google Scholar]
- Gu, L. Study on Single Disease of DRGs Based on Hospitalization Expenses in Cholecystitis Patients; Tianjin Medical University: Tianjin, China, 2013. [Google Scholar]
- Guo, S. Analysis of Hospital Costs Structure and Related Factors of Cholecystectomy Patients; Anhui Medical University: Hefei, China, 2004. [Google Scholar]
- He, W.Y. Analysis of Hospital Costs Structure and Related Factors of Single Diseases in a Grade III-A Hospital in Yunnan Provinces—Gallbladder Stone with Chronic Cholecystitis as Example; Kunming Medical University: Kunming, China, 2015. [Google Scholar]
- Botaitis, S.; Polychronidis, A.; Pitiakoudis, M.; Perente, S.; Simopoulos, C. Does gender affect laparoscopic cholecystectomy? Surg. Laparosc. Endosc. Percutaneous Tech. 2008, 18, 157–161. [Google Scholar] [CrossRef]
- Jiang, L.; Qin, D.; Kong, Q.; Li, B.; Qiu, S.; Yuan, X.; Shi, C. Hospitalization Expenses Analysis on Patients With of Single Disease Payment Basing on DRGs: A Case Study of Acute Calculous Cholecystitis. China Health Stand. Manag. 2019, 10, 14–16. [Google Scholar]
- Liu, X. Research on the Application of DRGs Technology in Hospital Operation and Management. China High New Technol. 2020, 17, 152–153. [Google Scholar]
- Meng, X. Effect of Diagnosis Related Groups (DRGs) Based Payment—An Experimental Study Based on the Pilot Reform in Sanming; China Medical University: Shenyang, China, 2020. [Google Scholar]
- Wu, X.; Li, J.; Deng, S.; Lin, L.; Tang, Y. Effect of DRGs payment reform on hospitalization costs of medical insurance patients in panzhihua city. Chongqing Med. 2021, 50, 4283–4287. [Google Scholar]
- Zhang, X.; Zhang, L. Intervention effects of pharmacists′ participation in clinical pathways on the rationality of patients′ medication under the DRGs payment model. Proceeding Clin. Med. 2022, 31, 459–462. [Google Scholar]
- Zhou, Y. Evaluation on the Implementation Effect of the Policy of Payment by Disease for Cancer Patients in N City Cancer Hospital; Yunnan University of Finance and Economics: Kunming, China, 2022. [Google Scholar]
- Zou, Q. Analysis of the Effect of Piloting C-DRG in A Large Comprehensive Tertiary Hospital in Shenzhen; Anhui Medical University: Hefei, China, 2020. [Google Scholar]
- Tang, J.; Song, L.; Zhang, T.; Xu, X.; Chen, W. Evaluation of DRGs Charging and Payment Simulation Operation Effect in A Hospital in Beijing. Chin. Health Qual. Manag. 2020, 27, 47–50. [Google Scholar]
- Zhou, W.; Yue, Y. Study on the Effect of Disease Related Group Payment on the Total Cost of Inpatients. Chin. J. Health Stat. 2019, 36, 261–263. [Google Scholar]
- Zhou, Z. Research on the Effect of DRGs Payment on the Control of Inpatient Medical Expenses—Take Tertiary Hospital as Example; East China University of Political Science and Law: Shanghai, China, 2021. [Google Scholar]
- Jian, W.Y.; Hu, M.; Jian, W.J.; Zhang, X. Evaluation on the Comprehensiveness of Diagnosis and Treatment Capacity Based on Diagnosis Related Groups. Chin. Hosp. Manag. 2010, 30, 17–19. [Google Scholar]
- Liu, R.; Shi, J.; Yang, B.; Jin, C.; Sun, P.; Wu, L.; Yu, D.; Xiong, L.; Wang, Z. Charting a path forward: Policy analysis of China’s evolved DRG-based hospital payment system. Int. Health 2017, 9, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Mo, X. Research progress in single disease management. Stat. Manag. 2016, 8, 117–118. [Google Scholar]
- Pan, Y.; Wang, M.; He, Z.; Meng, X.; Yang, L.; Xing, M. Research Progress and Countermeasures of Disease Diagnosis Related Groups at Home and Abroad. China J. Pharm. Econ. 2022, 17, 118–123+128. [Google Scholar]
- Wang, W.; Jia, X.; Zhou, D.; Zhong, X.; Wang, H. Study on DRG Operation Efficiency of Clinical Departments Based on DEA-BCC Model. Chin. J. Health Inform. Manag. 2023, 20, 652–657,665. [Google Scholar]
- Wu, S.; Lin, M.; Wu, X.; Lin, L.; Su, Z. Study on Influencing Factors and Operation Efficiency of Surgery Departments in a Certain Tertiary Hospital under DRG Payment Reform. Jiangsu Health Syst. Manag. 2023, 34, 357–360. [Google Scholar]
- Han, F.; Hu, W.; Zhao, J. Comparison of DRGs-PPS with DIP from the hospital perspective. Chin. Rural. Health Serv. Adm. 2021, 41, 864–868. [Google Scholar]
Figure 1.
Distribution of SDP studies by years and diseases.

Figure 2.
Flow chart of SDP study selection.

Figure 3.
Flow chart of DRG study selection.

Table 1.
Efficiency of SDP.
| First Author | Disease/Operation | Province | Number | Total Expenditure (RMB) | LOS (Day) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Post- SDP | Pre- SDP | Post- SDP | Pre- SDP | p Value | Post- SDP | Pre- SDP | p Value | |||
| Tang (2019) [9] | Laparoscopic cholecystectomy | Shandong | 266 | 202 | 13,858.32 | 21,699.15 | 0.00 | 4.70 | 8.31 | 0.02 |
| Sun (2019) [12] | Laparoscopic cholecystectomy | Hunan | 75 | 260 | 10,533.79 | 13,355.16 | <0.01 | 5.00 | 6.00 | <0.01 |
| Zhou (2018) [17] | Cholelithiasis with acute cholecystitis (Operation) | Yunnan | 27 | 30 | 5859.34 | 6264.37 | 0.05 | 6.49 | 7.47 | 0.16 |
| Zhou (2018) [17] | Cholelithiasis with acute cholecystitis (No Operation) | Yunnan | 44 | 51 | 3473.20 | 3537.37 | 0.66 | 5.48 | 6.06 | 0.03 |
| Zhang (2018) [18] | Laparoscopic cholecystectomy | Liaoning | 3864 | 4037 | 21,738.00 | 24,304.00 | <0.01 | 10.10 | 10.23 | 0.35 |
| Chen (2016) [10] | Cholelithiasis with acute cholecystitis | Anhui | 755 | 940 | 5550.80 | 6026.00 | 0.00 | 6.55 | 9.04 | 0.00 |
| Sun (2015) [11] | Laparoscopic cholecystectomy | Jiangsu | 23 | 23 | 9372.58 | 11,653.52 | <0.05 | 7.13 | 9.85 | <0.05 |
| Wang (2013) [13] | Laparoscopic cholecystectomy | Shandong | 50 | 50 | 4073.35 | 9887.13 | <0.01 | 5.00 | 13.00 | <0.01 |
| Yu (2012) [15] | Laparoscopic cholecystectomy | Jilin | 88 | 119 | 12,534.38 | 16,716.18 | <0.01 | 5.00 | 7.00 | <0.01 |
| Kong (2011) [14] | Laparoscopic cholecystectomy | Jiangsu | 100 | 100 | 3989.34 | 6321.88 | <0.05 | 4.40 | 6.80 | <0.05 |
| Su (2011) [21] | Laparoscopic cholecystectomy | Hunan | 383 | 516 | 5017.84 | 11,355.93 | <0.01 | 8.20 | 12.85 | 0.00 |
| Liu (2009) [19] | Laparoscopic cholecystectomy | Jilin | 139 | 163 | 8100.00 | 9900.00 | <0.01 | 5.80 | 8.20 | <0.01 |
| Jiang (2009) [18] | Laparoscopic cholecystectomy | Hubei | 95 | 91 | 5483.83 | 6470.44 | <0.05 | 8.20 | 10.50 | <0.05 |
| Ren (2006) [20] | Laparoscopic cholecystectomy | Hebei | 118 | 118 | 4390.00 | 5533.00 | <0.05 | 4.00 | 7.00 | <0.05 |
Table 3.
DRG grouping scheme of cholecystectomy implemented in Qilu hospital.
| DRG Code | DRG Group | RW | Number of Cases |
|---|---|---|---|
| HS10B | Laparoscopic cholecystectomy without common bile duct exploration | 0.95 | 2006 |
| HS10C | Laparoscopic cholecystectomy, day surgery | 0.95 | 2 |
| HS09C | Open cholecystectomy without exploration of common bile duct or severe complications | 1.66 | 82 |
| HS10A | Laparoscopic cholecystectomy with exploration of common bile duct | 1.75 | 78 |
| HS10 + HO03 | Complex treatment of laparoscopic cholecystectomy + ERCP | 1.77 | 52 |
| HS09A | Open cholecystectomy with exploration of common bile duct | 2.05 | 16 |
| HS09B | Open cholecystectomy with exploration of common bile duct and severe complications | 2.05 | 8 |
Table 4.
The efficiency of DRG in cholecystitis-related disorders.
| DRG Groups | RW | Number | LOS (Days) | Total Expenditure (RMB) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Pre- DRG | Post- DRG | Pre- DRG | Post- DRG | Difference | Pre- DRG | Post- DRG | Difference | ||
| Major surgery of biliary tract, with malignant tumor | 2.54 | 28 | 50 | 18.54 | 16.52 | 2.02 | 80,940.56 | 80,544.06 | 396.50 |
| Complex operations of ERCP, with severe complications and concomitants | 2.16 | 18 | 49 | 9.00 | 9.80 | −0.80 | 29,208.42 | 33,511.80 | −4303.38 |
| Other minor hepatobiliary and pancreatic surgery | 2.09 | 37 | 124 | 9.41 | 5.07 | 4.34 | 18,188.37 | 13,832.44 | 4355.92 |
| Percutaneous bile duct therapeutic procedure | 1.80 | 69 | 68 | 10.19 | 8.73 | 1.46 | 26,044.01 | 20,340.31 | 5703.70 |
| Laparoscopic cholecystectomy, with exploration of common bile duct | 1.75 | 16 | 20 | 14.00 | 11.70 | 2.30 | 43,822.88 | 44,061.44 | −238.56 |
| Laparotomic cholecystectomy, without exploration of common bile duct, without severe complications and concomitants | 1.66 | 18 | 17 | 13.56 | 15.18 | −1.62 | 48,591.35 | 54,390.31 | −5798.96 |
| Major surgery of biliary tract, without malignant tumor, with moderate complications and concomitants | 1.46 | 10 | 13 | 14.20 | 13.77 | 0.43 | 43,288.88 | 53,139.44 | −9850.56 |
| Complex operations of ERCP, without severe complications and concomitants | 1.38 | 81 | 149 | 8.37 | 7.23 | 1.14 | 25,374.83 | 24,181.43 | 1193.40 |
| Major surgery of biliary tract, without malignant tumor, without complications and concomitants | 1.15 | 44 | 43 | 12.82 | 10.00 | 2.82 | 38,133.45 | 36,957.94 | 1175.50 |
| Diagnostic operations of hepatobiliary system without severe complications and concomitants | 1.06 | 21 | 45 | 7.29 | 6.91 | 0.38 | 12,986.78 | 13,025.49 | −38.71 |
| Laparoscopic cholecystectomy, without exploration of common bile duct | 0.95 | 540 | 804 | 7.49 | 6.21 | 1.28 | 23,612.10 | 22,852.57 | 759.53 |
| Malignant tumor of liver, gallbladder, or pancreas, without severe complications and concomitants | 0.85 | 154 | 47 | 9.92 | 7.63 | 2.28 | 27,536.63 | 15,523.52 | 12,013.11 |
| Acute biliary tract disease, with complications and concomitants | 0.81 | 14 | 16 | 7.89 | 7.69 | 0.20 | 16,830.59 | 16,415.66 | 414.93 |
| Chronic biliary tract disease, with complications and concomitants | 0.70 | 18 | 22 | 6.66 | 5.32 | 1.34 | 10,504.02 | 8408.61 | 2095.41 |
| Acute biliary tract disease, without complications and concomitants | 0.64 | 30 | 25 | 7.57 | 5.84 | 1.73 | 15,092.63 | 8649.21 | 6443.42 |
| Chronic biliary tract disease, without complications and concomitants | 0.40 | 74 | 74 | 7.09 | 5.12 | 1.98 | 8267.54 | 6602.42 | 1665.12 |
Difference is obtained by subtracting the value of “post-DRG” group from the value of “pre-DRG” group.
Table 5.
The efficiency of DRG.
| First Author | DRGs | Province | Number | TE (RMB) | LOS (Day) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Post- DRG | Pre- DRG | Post- DRG | Pre- DRG | p Value | Post- DRG | Pre- DRG | p Value | |||
| Liu (2020) [29] | Local DRG | Henan | 9381 | 10,176 | 22,738 | 25,837 | <0.05 | 13.30 | 15.80 | <0.05 |
| Meng (2020) [30] | CN-DRG | Guangdong | 439,114 | 300,538 | 5301 | 5633 | <0.001 | 8.85 | 8.81 | <0.001 |
| Meng (2020) [30] | C-DRG | Guangdong | 232,255 | 300,538 | 5681 | 5633 | <0.001 | 8.70 | 8.81 | <0.001 |
| Zhou (2022) [33] | Local DRG | Yunnan | 23,887 | 165,261 | 14,819 | 17,435 | <0.001 | N/A | N/A | N/A |
| Tang (2020) [35] | CN-DRG | Beijing | 5982 | 2871 | 20,674 | 19,960 | 0.139 | 9.98 | 10.14 | 0.044 |
| Zhou (2021) [37] | CHS-DRG | Zhejiang | 24,728 | 18,355 | 10,125 | 9720 | <0.01 | 7.00 | 7.00 | <0.01 |
| Zhou (2019) [36] | Local DRG | Liaoning | 995 | 2165 | 19,048 | 17,510 | <0.01 | N/A | N/A | N/A |
| Zhang (2022) [32] | Local DRG | Hubei | 62 | 65 | 12,437 | 18,032 | 0.058 | 8.19 | 8.80 | 0.058 |
| Wu (2021) [31] | Local DRG | Sichuan | 12,019 | 11,533 | 8658 | 10,951 | <0.05 | 8.78 | 10.66 | <0.05 |
| Zou (2020) [34] | C-DRG | Guangdong | 237 | 234 | 11,739 | 12,278 | 0.725 | 4.87 | 5.34 | 0.019 |
Table 6.
Popular DRG versions in China.
| R&D Department | Year Published | Number of Groups (ADRG/DRGs) | RW | Character | |
|---|---|---|---|---|---|
| BJ-DRG | Beijing Medical Insurance Association | 2008 | 393/752 | Resource consumption | First localized DRG in China Focuses on expense control |
| CN-DRG | Beijing Municipal Health Commission | 2014 | 415/804 | Total expense of disease consumption | Focuses on medical performance evaluation and quality supervision |
| C-DRG | National Health Commission of the People’s Republic of China | 2015 | 455/958 | Total cost of disease consumption | Innovatively groups based on all disease spectra and CCHI |
| CHS-DRG | National Healthcare Security Administration | 2019 | 367/618 | Total cost of disease consumption | Refers to and integrates all above versions |
Adjacent-DRG (ADRG), the secondary classification in DRG system, groups cases mainly according to diagnosis and operations based on the broad categories verified by primary classification of major diagnostic categories (MDCs), while the tertiary classification diagnosis-related groups (DRGs) subdivides cases on this basis.
Table 7.
Comparison of SDP, DRG and DIP.
| SDP | DRG | DIP | |
|---|---|---|---|
| Payment | Prospective payment | Prospective payment | Prospective payment |
| Data source | Medical records | Medical records | Medical records |
| Grouping objects | Simple diseases with no comorbidities and complications | All diseases | All hospitalized patients |
| Payment standard | Categories of disease | Groups and Relative Weights | Groups and budget point value |
| Standardized | No | Only MDC and ADRG are standardized | Yes |
| Grouping pathway | N/A | Induction | Exhaustive method |
| Grouping basis | N/A | Clinical pathway | Clinical data |
| Grouping refinement | N/A | Similar diagnoses and operations in one group | Different diseases and operations in different groups |
| Intra-group differences | N/A | Significant | Insignificant |
| Number of groups | N/A | Usually less than 1000 | More than 10,000 |
| Requirement of medical record quality | Low | High | Low |
| Applying difficulty | Easy | Hard | Easy |
| Usage of big data | No | No | Yes |
MDC: Major Diagnostic Category, ADRG: Adjacent-DRG.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ma, W.; Qu, J.; Han, H.; Jiang, Z.; Chen, T.; Lu, X.; Lu, J. Statistical Insight into China’s Indigenous Diagnosis-Related-Group System Evolution. Healthcare 2023, 11, 2965. https://doi.org/10.3390/healthcare11222965
AMA Style
Ma W, Qu J, Han H, Jiang Z, Chen T, Lu X, Lu J. Statistical Insight into China’s Indigenous Diagnosis-Related-Group System Evolution. Healthcare. 2023; 11(22):2965. https://doi.org/10.3390/healthcare11222965
Chicago/Turabian StyleMa, Wenlong, Jing Qu, Hui Han, Zixia Jiang, Tiantian Chen, Xuefeng Lu, and Jiaoyang Lu. 2023. "Statistical Insight into China’s Indigenous Diagnosis-Related-Group System Evolution" Healthcare 11, no. 22: 2965. https://doi.org/10.3390/healthcare11222965
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.